Scar Wars
Ashley Wysong, MD, MS
Professor and Founding Chair, William W. Bruce, MD Distinguished Chair of Dermatology, Department of Dermatology, University of Nebraska Medical Center (UNMC)
June 2024

Dr. Wysong presented information about scar assessment and treatment.
First, Dr. Wysong discussed managing patient expectations for scar treatment. Scars are an outcome of the natural healing process when fibrous tissue replaces normal skin after skin injury. Patients should understand that their skin will never be exactly the same. Dr. Wysong makes sure to ask about personal or family history of poor scarring and to identify asymmetries or irregularities pre-operatively. She clearly communicates expectations about the healing process. It can take 12–18 months for skin to completely heal, and increased redness is normal.
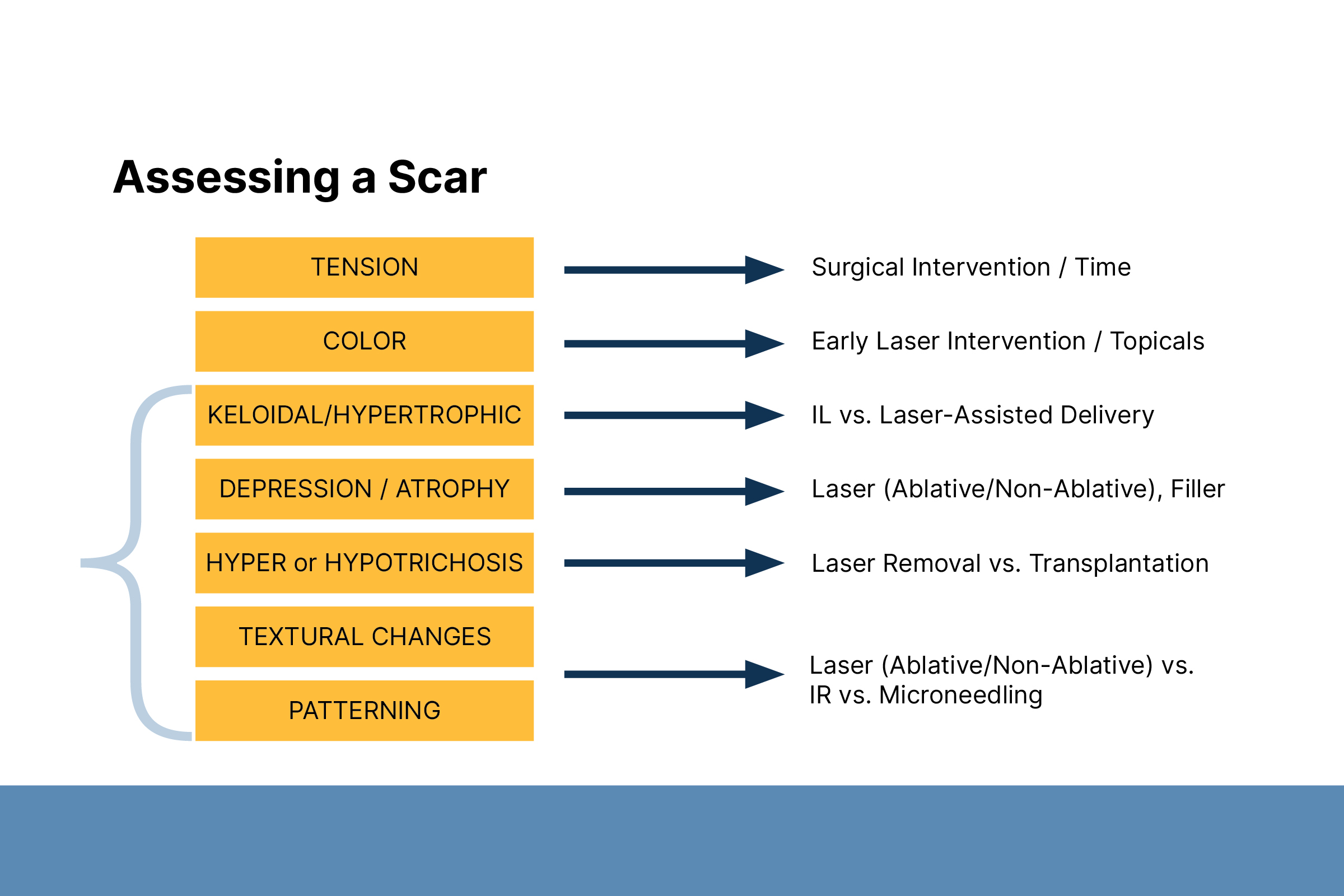
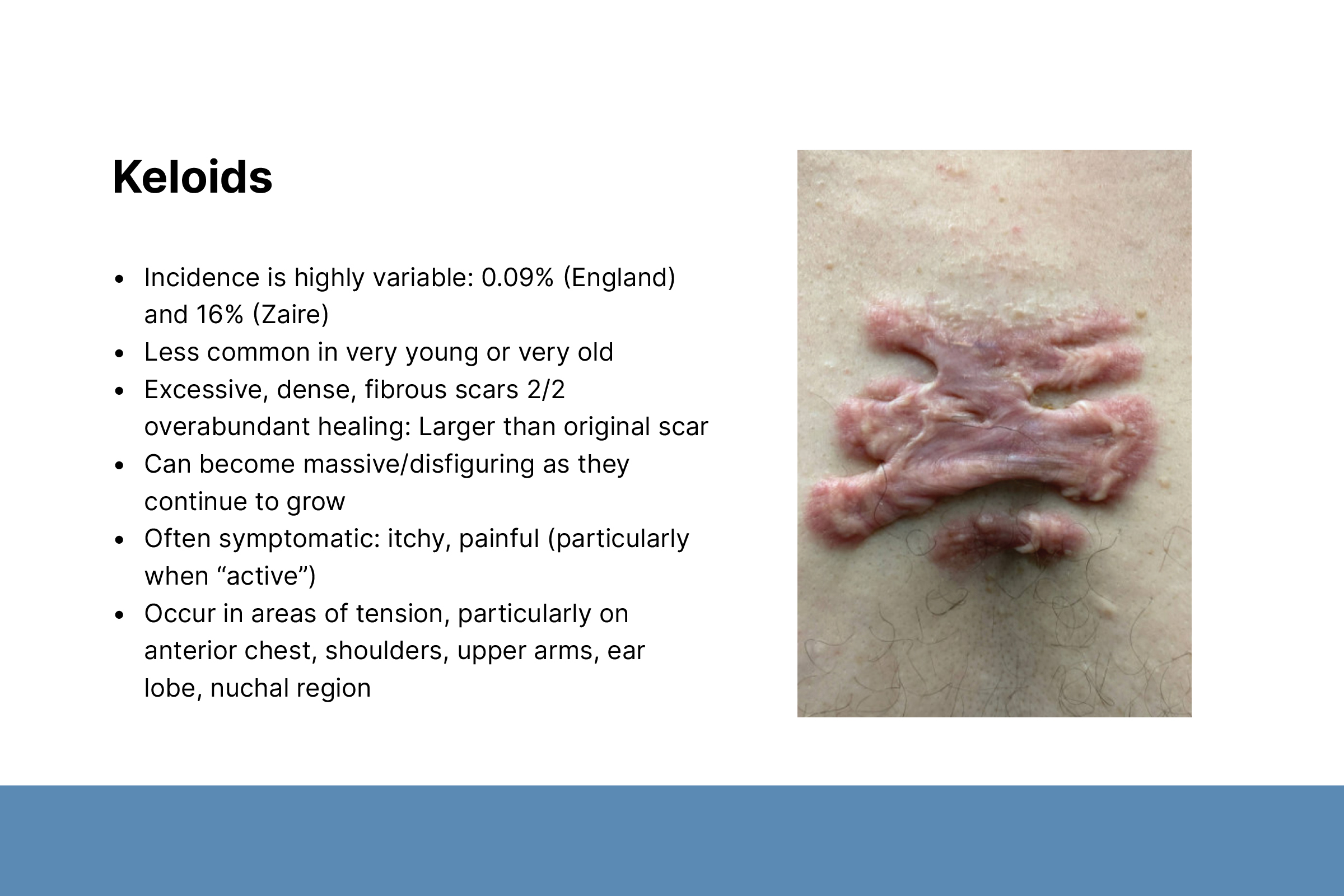
Second, Dr. Wysong described scar assessment based on tension, color, and texture. Tension occurs in mobile areas and plays a role in hypertrophic scars and keloidal processes. Discoloration includes hyperpigmentation, hypopigmentation, and erythema (redness).
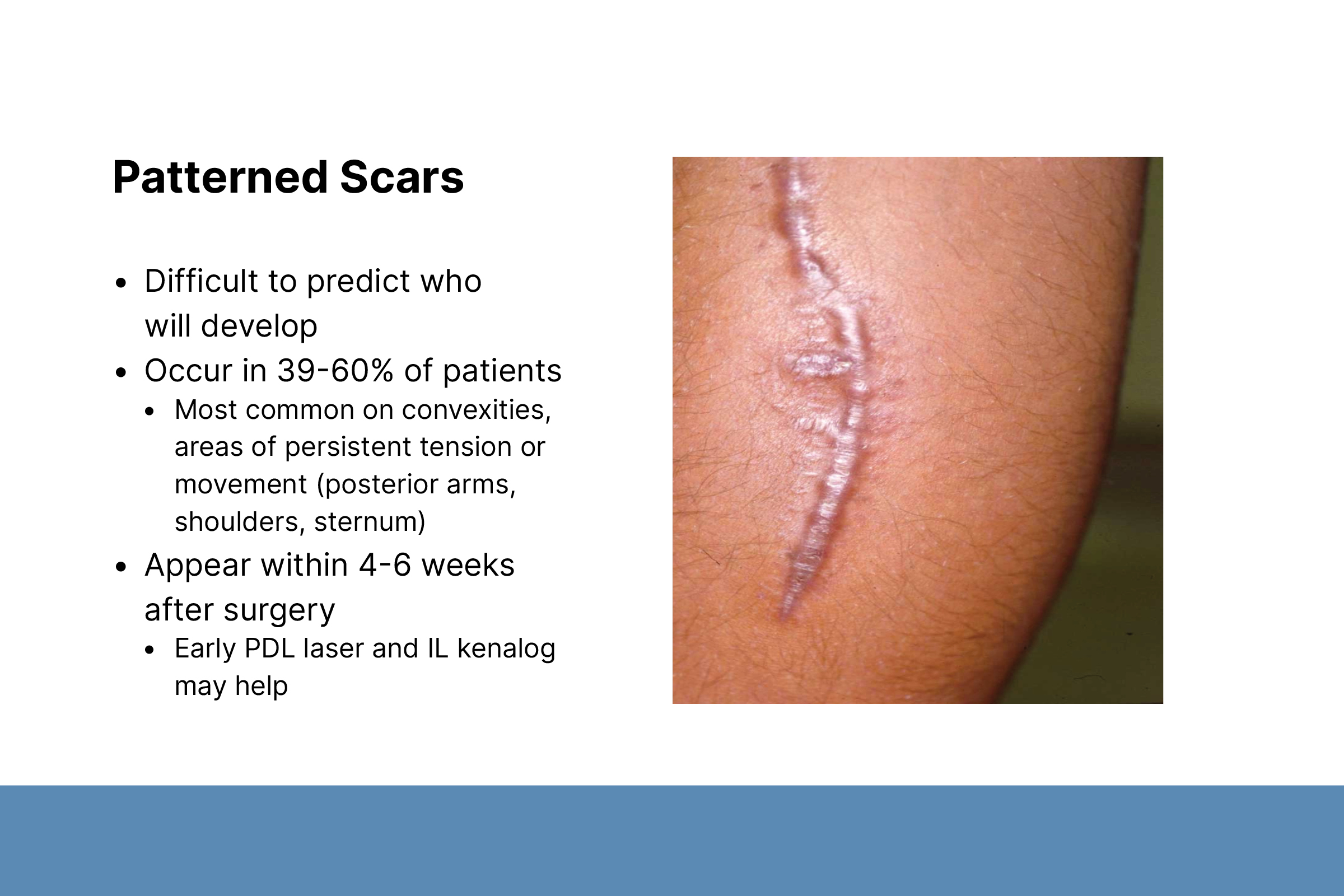
Scar textures include hypertrophic/keloidal, depressed/atrophic, and patterning. Hypertrophic/keloidal scars appear four to six weeks after surgery and occur in 39–60% of patients. Depressed/atrophic scars are commonly caused by acne, varicella, trauma, and poor surgical technique. They can be associated with hypopigmentation or depigmentation. Patterned scars can be caused by split-thickness skin graft meshing, as seen after trauma-related scars or burns.
Third, Dr. Wysong discussed treatment options, including topical medications, intralesional medications, surgical revision, and laser therapy. Scars under tension require longer wait times or surgical intervention to release the tension. Discoloration can be treated with topical medications and early laser interventions. Dr. Wysong described best practices for using topical and intralesional medications.
Fourth, Dr. Wysong discussed the use of different lasers for specific purposes. She recommended lasers that take advantage of hemoglobin chromophores for erythematous scars. Q-switch and picosecond lasers can be used for hyperpigmented scars.
Non-ablative or ablative CO2 lasers are used for irregular textures, hypertrophic, and keloidal scars. Non-ablative lasers remodel the dermis while keeping the epidermis intact. They can be used for surgical scars three to six months after surgery, acne scars, and patients who want shorter recuperation time. Non-ablative lasers are safe in patients with skin of color. Dr. Wysong typically uses CO2 ablative lasers with a combination of fractionated deep (5% density) and superficial modes depending on scar features. Very low-density fractionation or a radiofrequency microneedling bipolar device can be used on darker Fitzpatrick skin types.